
The Gut-Systemic Axis: Why Digestion, Barrier Integrity, and Microbial Balance Determine Whole-Body Health
Jul 03, 2026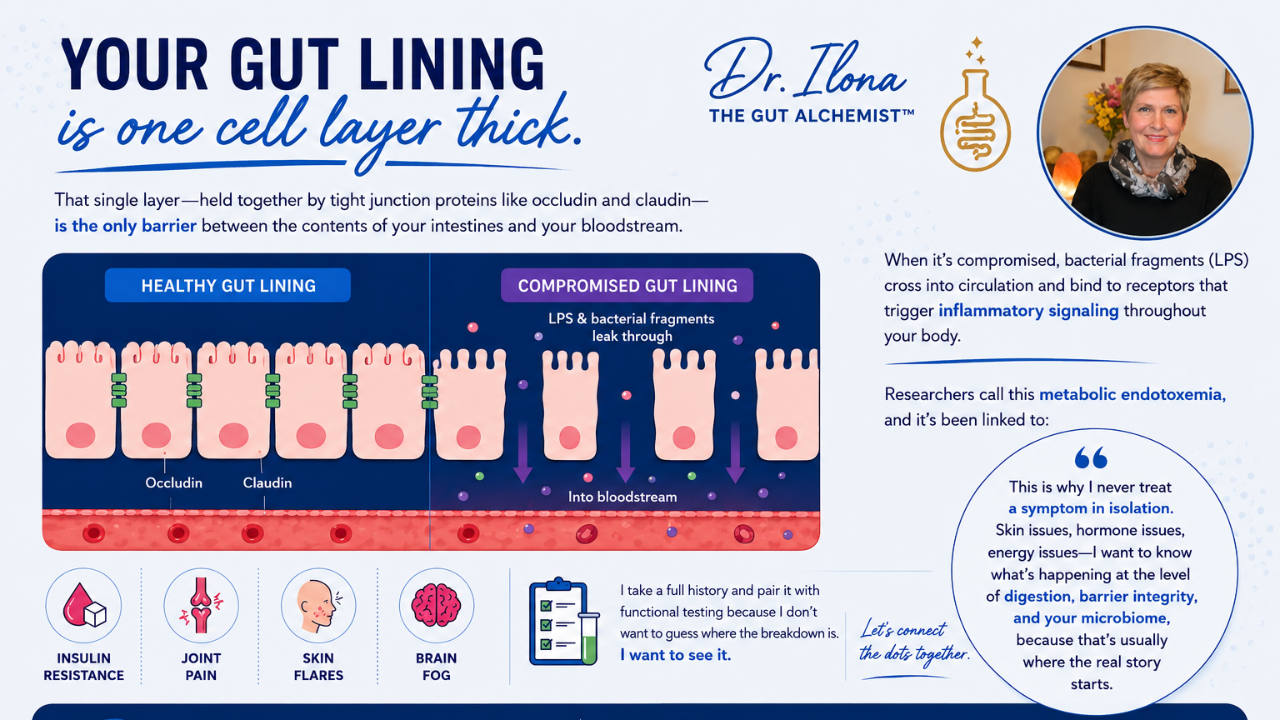
For decades, conventional medicine has treated the gastrointestinal tract as a somewhat isolated system — relevant to digestion, and little else.
Skin conditions went to dermatology.
Mood disorders went to psychiatry.
Autoimmune conditions went to rheumatology.
Metabolic conditions went to endocrinology.
Each specialty, working in its own silo, on what is often the same underlying process expressing itself in different tissues.
Having practiced in general medicine, emergency medicine, and dermatology before moving into functional medicine, I've observed this pattern from both sides of the exam room.
What I want to walk through here is the physiological rationale for why "gut health" is not a wellness buzzword — it is a mechanistically defensible framework for understanding a wide range of chronic, seemingly unrelated symptoms.
I organize this around three interdependent pillars:
- Digestive function
- Intestinal barrier integrity
- Microbial ecology
A disruption in any one propagates through the other two, and from there, systemically.
Digestive Function
Digestion is frequently reduced to "stomach acid and enzymes," but it begins upstream, in the cephalic phase — the anticipatory, vagally-mediated response to the sight, smell, or thought of food, which primes gastric acid secretion, pancreatic enzyme output, and biliary flow.
Chronic sympathetic activation (stress, eating while distracted, irregular meal timing) blunts this phase, reducing downstream digestive capacity before a meal has even begun.
Clinically, low gastric acid output (hypochlorhydria) is underdiagnosed relative to hyperacidity, particularly with advancing age, chronic stress, H. pylori colonization, and long-term proton pump inhibitor use.
Adequate gastric acidity is required for:
- Pepsinogen activation
- Mineral solubility
- Signaling downstream pancreatic secretion
- Signaling biliary secretion
Insufficient acid output produces a cascade:
- Impaired protein hydrolysis
- Reduced enzymatic and bile signaling
- Delayed gastric emptying
- Bacterial overgrowth from undigested substrate
This is the mechanistic basis for much of what patients describe as post-meal bloating and fullness.
Intestinal Barrier Integrity
The intestinal epithelium is a single layer of cells linked by tight junction protein complexes — occludin, claudins, and zonula occludens proteins — which regulate paracellular permeability.
Zonulin, a modulator of tight junction assembly, has been identified as one mechanism by which permeability increases in response to triggers such as gliadin exposure, dysbiosis, and pro-inflammatory cytokine signaling.
When barrier integrity is compromised, bacterial lipopolysaccharide (LPS) and other luminal antigens gain access to the lamina propria and systemic circulation.
LPS is a potent agonist of Toll-like receptor 4 (TLR4), triggering NF-κB-mediated production of pro-inflammatory cytokines (TNF-α, IL-6, IL-1β).
This process — termed metabolic endotoxemia when chronic — has been implicated in a wide range of downstream conditions, from insulin resistance to neuroinflammation to autoimmune activation, depending on individual genetic and environmental susceptibility.
This is the mechanistic link between "leaky gut" and the seemingly unrelated presentations practitioners see daily:
- Joint pain
- Cognitive fog
- Skin eruptions
- Fatigue
Symptoms that often resist explanation when the gut is never examined as the source.
Microbial Ecology
The gut microbiota functions as a metabolically active endocrine-adjacent organ.
Several mechanisms are worth highlighting.
The Gut-Brain Axis
An estimated 90% of the body's serotonin is synthesized in enterochromaffin cells of the gut, influenced by microbial metabolites.
Short-chain fatty acids (SCFAs), particularly butyrate, produced through bacterial fermentation of dietary fiber, serve as the primary energy substrate for colonocytes, support tight junction protein expression, and exert systemic anti-inflammatory and neuromodulatory effects via vagal afferent signaling.
The Estrobolome
A specific subset of gut bacteria expressing beta-glucuronidase deconjugates hepatically-processed estrogens, permitting their reabsorption rather than excretion.
Dysbiosis with elevated beta-glucuronidase activity is associated with increased circulating estrogen — a mechanism relevant to estrogen-dependent conditions including endometriosis and certain hormone-sensitive presentations.
Metabolic Regulation
Microbial diversity and composition influence energy harvest from the diet, SCFA-mediated insulin sensitivity, and bile acid signaling through FXR and TGR5/GPBAR1 receptors — pathways increasingly implicated in the pathophysiology of insulin resistance and metabolic dysfunction-associated steatotic liver disease (MASLD).
Clinical Implications
These three pillars do not operate independently.
Impaired digestion increases luminal substrate available for dysbiotic fermentation.
Dysbiosis reduces SCFA production, compromising the very tight junction integrity that maintains the barrier.
Barrier compromise drives the systemic inflammatory signaling that feeds back to impair digestive and microbial function further.
It is a closed loop, not a linear chain — which is precisely why isolated, symptom-specific interventions so often fail to produce durable results.
This is the rationale behind a root-cause approach:
A thorough clinical history to identify where in this loop the disruption likely originated, paired with targeted functional testing — stool analysis, organic acids, hormone panels — to confirm mechanism rather than assume it.
If a patient's chronic symptoms have resisted resolution through single-specialty, single-symptom approaches, the gut-systemic axis is worth clinical consideration — not as an alternative to conventional diagnostics, but as a frequently overlooked layer beneath them.
To your radiant health and thriving gut,
Dr. Ilona