
By Dr Ilona Horti Berkoben | The Gut Health Revolution
Introduction
Every week I sit with patients who arrive carrying folders of diagnoses, prescriptions and specialist referral letters.
Type 2 Diabetes.
Cardiovascular disease.
Autoimmune conditions.
Chronic fatigue.
Brain fog that has stolen years of their quality of life.
And almost universally, nobody has ever asked them the most important question of all:
Where did this actually begin?
Because here is the truth that conventional medicine rarely tells you: your diagnosis did not begin the day it was detected. It began years — sometimes decades — earlier. And in a growing number of cases, it began in the gut.
Specifically, it began with a breakdown of the intestinal barrier — a phenomenon increasingly documented in peer-reviewed literature and known clinically as intestinal hyperpermeability, or leaky gut.
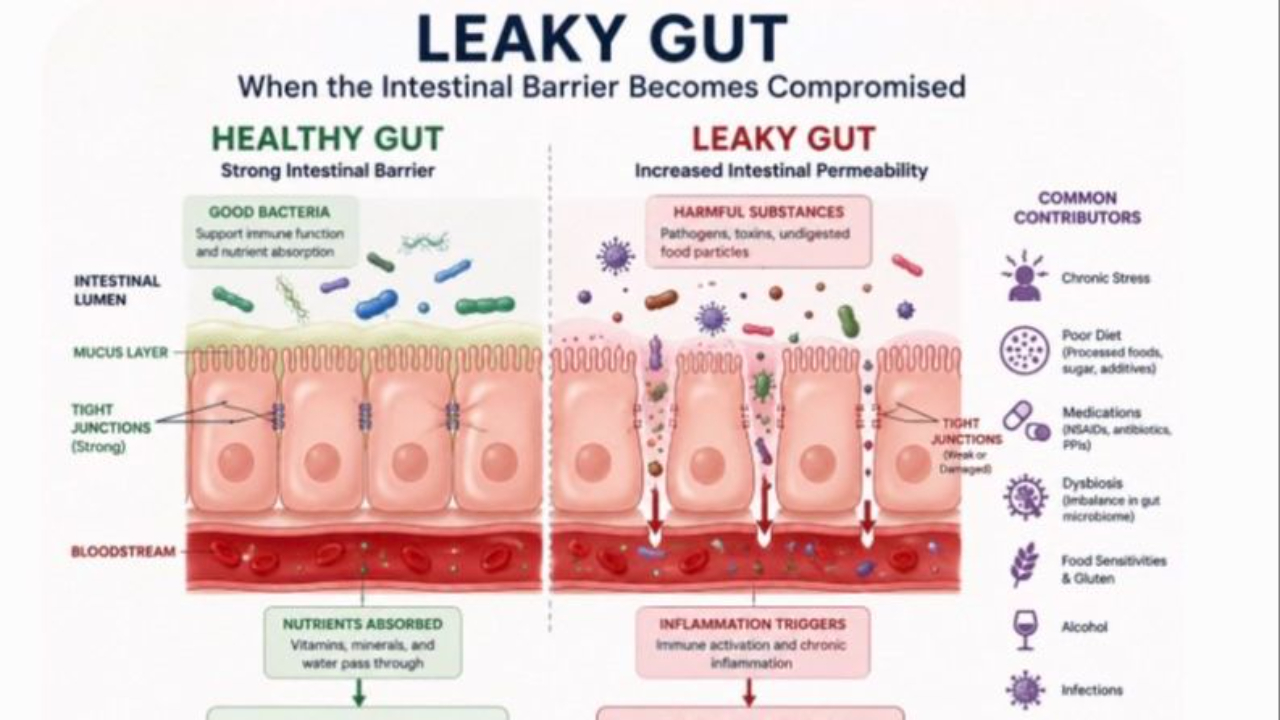
What Is Intestinal Hyperpermeability?
The intestinal lining is a remarkable structure.
It is precisely one cell thick — a single layer of epithelial cells called enterocytes — and yet it performs one of the most critical functions in the human body.
Its job is elegant in its simplicity:
Let the good in, keep the bad out.
Nutrients, vitamins and minerals pass through.
Toxins, undigested food particles and pathogens do not.
The integrity of this barrier depends on specialised protein complexes known as tight junctions — molecular gatekeepers that sit between the enterocytes and regulate what passes into systemic circulation.
The key proteins involved include:
- Zonulin — the primary regulator of tight junction permeability
- Occludin — a structural tight junction protein
- Claudins — a family of proteins essential to barrier function
- Actomyosin — involved in the mechanical opening and closing of tight junctions
When these proteins are functioning optimally, the barrier holds.
When they are chronically disrupted — by diet, medication, stress, infection or dysbiosis — the tight junctions loosen.
The barrier becomes permeable.
And when the barrier becomes permeable, the consequences are systemic.
The LPS Connection: Metabolic Endotoxemia
At the centre of the leaky gut story is a molecule called lipopolysaccharide (LPS).
LPS is a component of the outer membrane of gram-negative bacteria — the kind that normally reside in large numbers in the gut.
Under healthy conditions, LPS stays in the gut where it belongs.
But when intestinal permeability increases, LPS translocates into the bloodstream.
This condition is called metabolic endotoxemia.
The immune system responds to circulating LPS with a powerful inflammatory cascade, activating toll-like receptor 4 (TLR4) and triggering the release of pro-inflammatory cytokines including TNF-α, IL-1β and IL-6.
The result is chronic, low-grade systemic inflammation — the underlying driver of virtually every chronic disease we face today.
In a landmark 2007 study, Cani et al. published in the journal Diabetes demonstrated that metabolic endotoxemia — driven by elevated circulating LPS — was sufficient to initiate obesity, insulin resistance and metabolic inflammation in animal models.
This was a pivotal moment in understanding the gut-disease connection.
The Systemic Consequences of Leaky Gut
The research linking intestinal hyperpermeability to systemic disease is substantial and growing.
Here is what the evidence shows:
Insulin Resistance & Type 2 Diabetes
Elevated LPS directly impairs insulin signalling at the cellular level.
A 2011 study in Diabetologia found significantly higher levels of LPS-binding protein in patients with Type 2 Diabetes compared to healthy controls, suggesting chronic endotoxemia as a contributing driver.
Cardiovascular Disease
LPS-driven inflammation promotes endothelial dysfunction, arterial stiffness and atherosclerotic plaque formation.
Research published in the Journal of the American College of Cardiology has identified gut dysbiosis and increased intestinal permeability as independent risk factors for cardiovascular events.
Non-Alcoholic Fatty Liver Disease (NAFLD)
The liver is the first organ exposed to portal blood from the gut.
Chronic LPS translocation drives hepatic inflammation, fat accumulation and progression to NASH (non-alcoholic steatohepatitis).
Autoimmune Conditions
Dr. Alessio Fasano groundbreaking research at Harvard demonstrated that intestinal hyperpermeability is a prerequisite for the development of autoimmune disease — including Type 1 Diabetes, coeliac disease, multiple sclerosis and Hashimoto’s thyroiditis.
His 2012 paper in Clinical Reviews in Allergy & Immunology proposed the model:
Genetic predisposition + environmental trigger + leaky gut = autoimmune disease
Neuroinflammation: Brain Fog, Anxiety & Depression
Via the gut-brain axis, LPS-driven systemic inflammation crosses the blood-brain barrier and activates microglial cells — the brain’s immune cells.
This neuroinflammatory state is now strongly associated with:
- Depression
- Anxiety
- Cognitive decline
- Brain fog
A 2021 review in Frontiers in Psychiatry identified leaky gut as a significant contributor to neuropsychiatric conditions.
Joint Pain & Rheumatoid Arthritis
Circulating LPS and inflammatory cytokines accumulate in synovial tissue, driving joint inflammation.
Multiple studies have identified gut dysbiosis and increased intestinal permeability in patients with rheumatoid arthritis preceding joint symptoms.
The Timeline: Your Disease Started Years Before Your Diagnosis
This is perhaps the most important concept I share with my patients.
Chronic disease does not arrive suddenly.
It is the end point of a long, slow process — a cascade of compounding insults that the body compensates for, silently, until it can no longer do so.
Here is how the timeline typically unfolds:
Stage 1 — The First Insult
It begins quietly.
Perhaps as reflux.
Indigestion after meals.
Heartburn.
Nothing serious.
A PPI is prescribed. Symptoms resolve. Life continues.
But PPIs reduce gastric acid — the body’s primary defence against pathogenic bacteria.
Low stomach acid creates the perfect terrain for bacterial overgrowth.
Stage 2 — Or Perhaps It Was the Gallbladder
Years of sluggish bile flow.
Gallstones forming silently.
One day — a gallbladder removal.
The patient is told they will be fine without it.
But bile is not just for fat digestion.
It is antimicrobial.
Without adequate bile flow, the small intestine becomes vulnerable to bacterial colonisation — the foundation of SIBO.
Stage 3 — Dysbiosis Takes Hold
Whether triggered by PPIs, gallbladder removal, repeated antibiotics or a high sugar diet — the microbiome shifts.
Pathogenic bacteria proliferate.
Beneficial species decline.
The gut environment becomes hostile to a healthy lining.
Stage 4 — The Gut Lining Breaks Down
Chronic dysbiosis, combined with dietary triggers and stress, begins to compromise the tight junctions.
Zonulin is released.
The barrier opens.
LPS enters the bloodstream.
Metabolic endotoxemia begins.
Stage 5 — Years Later: The Diagnosis
Insulin resistance is detected.
Or cardiovascular markers worsen.
Or an autoimmune condition emerges.
Or the joints begin to ache.
And the patient is told they have a new disease.
But the disease was not new.
It had been building for years.
The body had been sending signals — fatigue, bloating, brain fog, skin issues — that were treated in isolation, never connected.
This is the story I help my patients rewrite.
Key Causes of Intestinal Hyperpermeability
The research identifies multiple contributors to tight junction disruption:
- Gluten — triggers Zonulin release in all individuals, not just those with coeliac disease (Fasano, 2012)
- NSAIDs — directly damage the intestinal lining with even short-term use
- PPIs — reduce gastric acid, promoting dysbiosis and bacterial overgrowth
- Antibiotics — devastate microbiome diversity, often with lasting effects
- Chronic psychological stress — elevates cortisol, which directly disrupts tight junction proteins
- High sugar & ultra-processed food diet — feeds pathogenic bacteria and promotes inflammation
- Alcohol — increases intestinal permeability within hours of consumption
- Environmental toxins — glyphosate has been shown to disrupt tight junctions
- SIBO & Candida overgrowth — produce metabolites toxic to the gut lining
Measuring Intestinal Permeability
Clinically, several markers can help assess gut barrier function:
- Serum Zonulin — elevated levels indicate tight junction disruption
- Occludin & Actomyosin antibodies — Cyrex Array 2 measures these directly
- LPS Binding Protein (LBP) — indirect marker of circulating LPS
- Secretory IgA (sIgA) — low levels indicate compromised mucosal immunity
- Calprotectin — marker of intestinal inflammation
- Food sensitivity panels — multiple simultaneous reactions suggest barrier compromise
The Path to Healing
The gut lining has a remarkable capacity for regeneration — enterocytes turnover every 3–5 days under optimal conditions.
With the right support, meaningful healing is possible.
Evidence-Based Interventions Include:
- L-Glutamine — the primary fuel source for enterocytes; supports tight junction repair
- Zinc Carnosine — demonstrated to stabilise the gut lining and reduce permeability
- Vitamin D — regulates tight junction proteins and modulates gut immune function
- Collagen & Bone Broth — rich in glycine, proline and hydroxyproline — structural components of the gut lining
- Removal of dietary triggers — particularly gluten, processed foods and alcohol
- Microbiome restoration — through targeted prebiotics and careful probiotic use
- Stress regulation — the gut-brain axis is bidirectional; chronic stress perpetuates leaky gut
Conclusion
Leaky gut is not a trend.
It is not a fringe concept.
It is a measurable physiological reality with documented connections to some of the most prevalent chronic diseases of our time.
The question we must begin asking — as practitioners and as patients — is not just:
What diagnosis does this person have?
But:
What happened in this person’s body years before the diagnosis was made?
Because when we find the root — we can truly begin to heal.
About Dr Ilona Horti Berkoben
Dr Ilona Horti Berkoben is a Functional Medicine Practitioner and founder of The Gut Health Revolution.
She specialises in root cause healing, gut health restoration and connecting the dots between chronic symptoms and systemic disease.
👉 To book a free 30 minute Clarity Call, visit drilona/gut-health-transformation-call
References
Cani PD et al. (2007). Metabolic endotoxemia initiates obesity and insulin resistance.
Diabetes, 56(7), 1761–1772.
Fasano A. (2012). Leaky gut and autoimmune diseases.
Clinical Reviews in Allergy & Immunology, 42(1), 71–78.
Fasano A. (2012). Zonulin, regulation of tight junctions, and autoimmune diseases.
Annals of the New York Academy of Sciences, 1258(1), 25–33.
Pendyala S et al. (2012). A high-fat diet is associated with endotoxemia that originates from the gut.
Gastroenterology, 142(5), 1100–1101.
Camara-Lemarroy CR et al. (2021). Intestinal permeability and neuropsychiatric disorders.
Frontiers in Psychiatry.